This study reported:
- In animal studies, α2δ-1 and its interactions with NMDA receptors in the spinal cord triggered the pain sensitivity and analgesic tolerance that occurs with chronic morphine treatment.
- Blocking the α2δ-1–NMDA interaction reduced opioid-induced hyperalgesia and analgesic tolerance.
People who take opioids for pain control over long periods of time can actually become more sensitive to pain—a phenomenon called hyperalgesia. They can also develop tolerance to the opioid’s analgesic effects. Together, these two effects dampen the response to opioids, which may prompt increases in opioid taking and enhances the risk of misuse and overdose. According to a recent NIDA-supported study, presynaptic N-methyl-d-aspartate (NMDA) receptors for the neurotransmitter glutamate in spinal cord neurons and a protein called α2δ-1 are crucial for the development of this hyperalgesia and analgesic tolerance. “We showed for the first time that inhibiting α2δ-1 activity—by using gabapentin, interrupting the α2δ-1–NMDA receptor complex, or genetically deleting the gene coding for α2δ-1—diminished opioid-induced hyperalgesia and analgesic tolerance,” explains Dr. Hui-Lin Pan, the study’s lead investigator.
Chronic Opioid Treatment Increases α2δ-1–NMDA Interaction
Previous studies had already linked presynaptic NMDA receptors in spinal cord neurons to opioid-induced hyperalgesia. Additionally, Dr. Pan’s research team had discovered that the α2δ-1 protein physically interacted with NMDA receptors and stimulated their activity. In their most recent study, Dr. Meichun Deng, Dr. Pan, and colleagues at the University of Texas MD Anderson Cancer Center investigated whether the α2δ-1–NMDA interaction is responsible for opioid-induced hyperalgesia and analgesic tolerance in rats and mice.
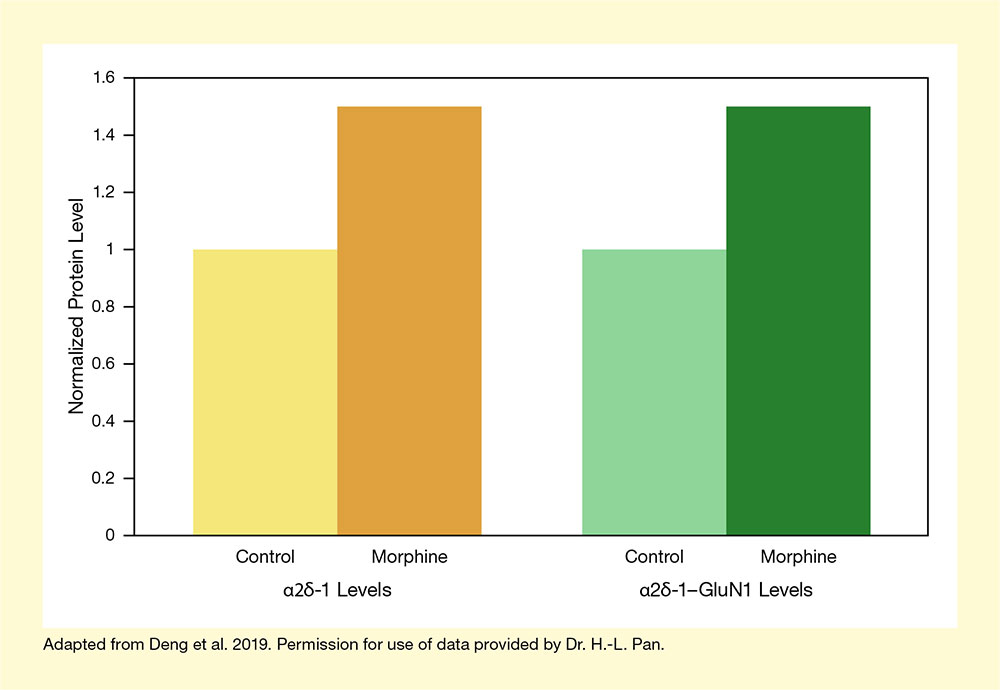
The investigators first examined how chronic opioid treatment affected the α2δ-1–NMDA interaction. These experiments showed that chronic morphine treatment increased NMDA receptor activity in spinal cord neurons, as well as both α2δ-1 levels and the protein’s physical interaction with NMDA receptors (see Figure 1). Stopping α2δ-1 from interacting with the NMDA receptor—by treating the neurons with either gabapentin or a blocking peptide—prevented this NMDA activation. Similarly, genetically modified mice that lacked the gene encoding α2δ-1, Cacna2d1, exhibited reduced NMDA activity in spinal cord neurons.
α2δ-1–NMDA Interactions Are Responsible for Excessive Pain Sensitivity and Tolerance
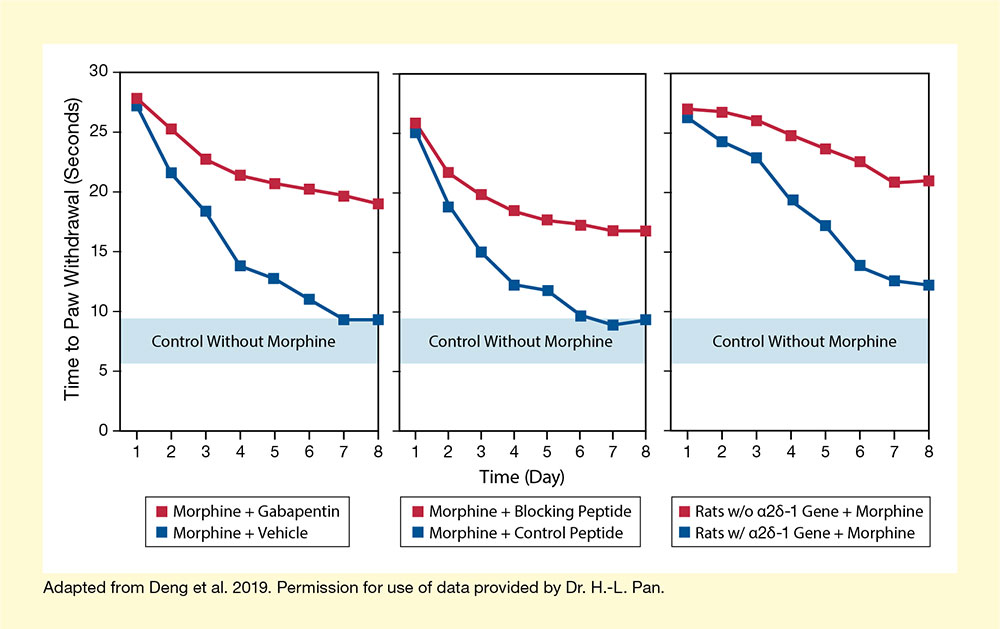
The research team then looked at whether blocking α2δ-1 altered pain sensitivity in rats receiving chronic morphine treatment. As expected, rats treated with morphine over 8 days gradually exhibited a lower pain threshold, signifying development of hyperalgesia and tolerance. However, when the rats were also treated with gabapentin or the α2δ-1 blocking peptide, the hyperalgesia abated. Likewise, the genetically modified mice that lacked the α2δ-1 gene did not develop hyperalgesia and showed reduced analgesic tolerance in response to chronic morphine treatment (see Figure 2).
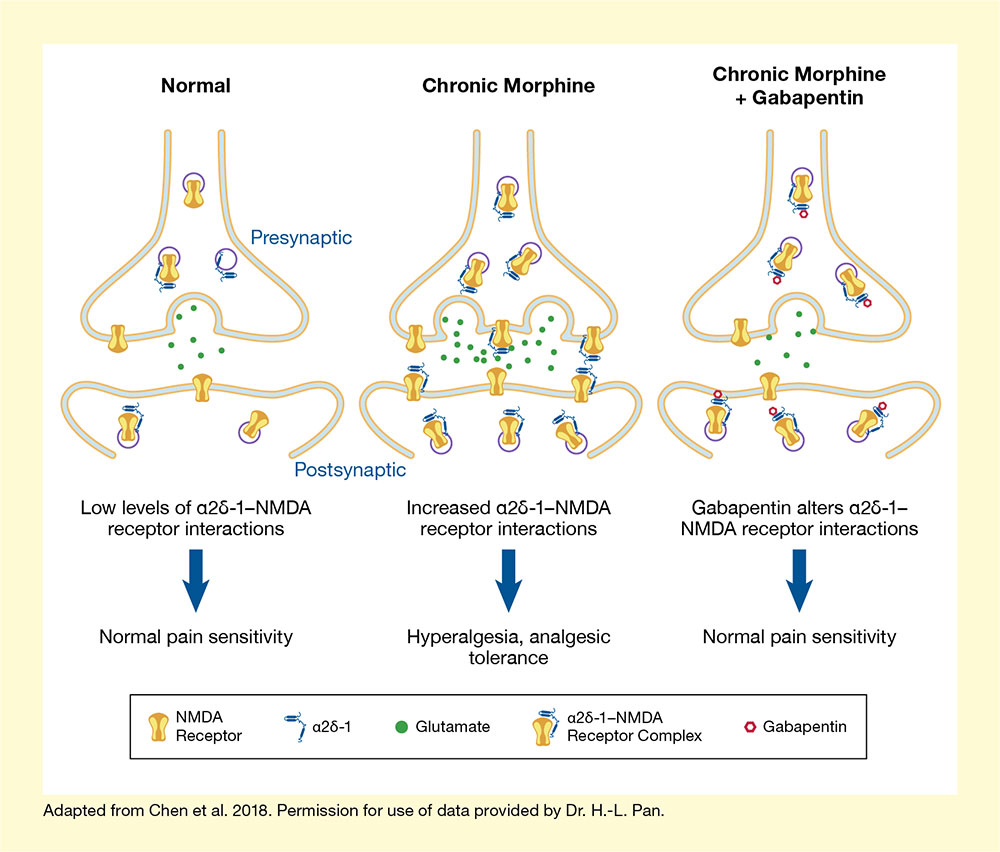
The findings indicate that the interaction between α2δ-1 and presynaptic NMDA receptors in spinal cord neurons is essential for the development of opioid-induced hyperalgesia and analgesic tolerance in rodents (see Figure 3). If future studies can confirm that α2δ-1 has the same effect in humans, strategies to block the α2δ-1–NMDA receptor interaction may help prevent the hyperalgesia and analgesic tolerance that develops in patients needing chronic opioid treatment for pain control. To design such strategies, the research team is working to determine the detailed protein structure of the α2δ-1–NMDA receptor complex. “This information will facilitate the design and development of more specific drugs that target α2δ-1–bound NMDA receptors for treating opioid-induced hyperalgesia and analgesic tolerance, drug addiction, and neuropathic pain.” explains Dr. Pan.
Dr. Pan also notes that their research to date has focused on α2δ-1–NMDA receptor interactions in the spinal cord. However, these interactions also occur in the brain. Therefore, the researchers plan to determine if and how α2δ-1–bound NMDA receptors in the brain contribute to other adverse effects of opioids, such as addiction.
This study was supported by NIDA grant DA041711.
- Caption and text description of Figure 1
-
Caption - (Left panel) Spinal cord tissues of rats that were treated with morphine for several days contained higher levels of α2δ-1 than did tissues from control animals. (Right panel) Similarly, the levels of α2δ-1 that physically interacted with NMDA receptors in the spinal cord was higher in the morphine-treated animals. Note: α2δ-1 levels in the control animals were set as 1.0.
Text Description - The bar chart shows the levels of α2δ-1 and α2δ-1–GluN1 levels in control rats and in animals chronically treated with morphine. Yellow bars represent α2δ-1 levels and green bars represent α2δ-1–GluN1 levels. Lighter bars represent control animals and darker bars represent morphine-treated animals, respectively. The vertical y-axis shows the normalized protein levels on a scale from 0 to 1.6. For both α2δ-1 and α2δ-1–GluN1, the values of the control animals are set as 1, and the values for the morphine-treated animals are 1.5
- Caption and text description of Figure 2
-
Caption - Rats were treated with morphine for 8 days and their pain sensitivity tested by exposing one of their paws to a heat source and measuring how soon the animals withdrew the paw (the maximum was 30 seconds to prevent potential tissue damage). Without any morphine treatment, animals would withdraw their paw after about 5 to 10 seconds (shaded area). Morphine treatment provided pain relief that progressively declined over the 8 days, indicating the presence of hyperalgesia and analgesic tolerance (blue curves). Concurrent treatment with gabapentin (left) or a blocking peptide (middle), as well as deletion of the gene encoding α2δ-1 (right) prevented or lessened hyperalgesia and tolerance (red curves).
Text Description - The three graphs show pain sensitivity of rats treated for 8 days with morphine with or without interventions to block α2δ-1 activity. Pain sensitivity was assessed by placing the animal’s paw on a hot plate and measuring the time until the animal withdrew the paw (the maximum time was 30 seconds to prevent tissue damage.) For all three charts, the horizontal x-axis shows the time in days and the vertical y-axis shows the time until paw withdrawal in seconds on a scale from 0 to 30. Light blue horizontal bars indicate the time to paw withdrawal for control animals not treated with morphine. In all cases, this was between 5 and 10 seconds throughout the experiment.
The left panel shows the data for animals treated with morphine with or without the α2δ-1 inhibitor gabapentin. The red curve shows pain sensitivity with gabapentin, the blue curve without gabapentin. For gabapentin-treated animals, time to paw withdrawal declined from about 28 seconds on day 1 to about 19 seconds on day 8, indicating a modest increase in pain sensitivity. For the animals not treated with gabapentin, the time to paw withdrawal dropped from about 28 seconds on day 1 to about 10 seconds on day 8, indicating a greater increase in pain sensitivity compared with gabapentin treatment.
The middle panel shows the data for animals treated with morphine with or without a blocking peptide that interferes with α2δ-1 activity. The red curve shows pain sensitivity with the blocking peptide, and the blue curve shows pain sensitivity with a control peptide. For blocking peptide-treated animals, time to paw withdrawal declined from about 26 seconds on day 1 to about 17 seconds on day 8, indicating a modest increase in pain sensitivity. For the animals treated with the control peptide, the time to paw withdrawal dropped from about 26 seconds on day 1 to about 10 seconds on day 8, also indicating a greater increase in pain sensitivity compared with the blocking peptide treatment.
The right panel shows the data for animals that lack the α2δ-1 gene or have a normal gene. The red curve shows the effect for animals lacking the α2δ-1 gene, the blue curve shows the effect for animals with a normal α2δ-1 gene. For the animals lacking the α2δ-1 gene, time to paw withdrawal declined from about 28 seconds on day 1 to about 22 seconds on day 8, indicating a slight increase in pain sensitivity. For the animals with the normal α2δ-1 gene, the time to paw withdrawal dropped from about 28 seconds on day 1 to about 12 seconds on day 8, indicating a greater increase in pain sensitivity compared with animals lacking the α2δ-1 gene.
- Caption and text description of Figure 3
-
Caption - Compared with normal conditions, chronic morphine treatment increases the levels of α2δ-1, as well as α2δ-1–NMDA receptor interactions, causing increased glutamate release from the presynaptic neuron. This activates the postsynaptic neuron, resulting in hyperalgesia and analgesic tolerance. If the α2δ-1–NMDA interaction is blocked, for example by treatment with gabapentin, glutamate release declines to normal levels and re-establishes normal pain sensitivity levels.
Text Description - The graphic illustrates the proposed mechanism through which the interaction of α2δ-1 with NMDA receptors mediates hyperalgesia. The three panels each show a presynaptic cell (top) and a postsynaptic cell (bottom). The yellow structures represent NMDA receptors that are embedded into the cell membrane or the membrane of internal vesicles. Small blue structures represent the α2δ-1 molecule that can interact with the NMDA receptor. Green dots represent glutamate molecules that are released into the space between the presynaptic and postsynaptic cell and can interact with NMDA receptors. In the normal state (left panel), there are low levels of α2δ-1–NMDA receptor interaction, resulting in low levels of glutamate release and normal pain sensitivity. With chronic morphine treatment (middle panel), there are more NMDA molecules, more α2δ-1 molecules, and more α2δ-1–NMDA complexes, and more glutamate is released into the space between the two cells. This in turn causes hyperalgesia and analgesic tolerance. The right panel shows the effects of chronic morphine treatment and concurrent treatment with gabapentin, indicated by red circles. Gabapentin binds to α2δ-1 and the α2δ-1–NMDA complexes. As a result, only low amounts of glutamate are released into the space between the two cells, and pain sensitivity returns to normal.
Source:
- Deng, M., Chen, S.R., Chen, H., Pan, H.L. α2δ-1-bound N-methyl-D-aspartate receptors mediate morphine-induced hyperalgesia and analgesic tolerance by potentiating glutamatergic input in rodents. Anesthesiology 130(5):804-819, 2019.