This study reported that:

- People with a substance use disorder (SUD) at any time in their lives are 1.5 times more likely to contract COVID-19 than those without an SUD, and those with a recent SUD are more than 8 times more likely.
- People with opioid use disorder (OUD) and African Americans are at particularly high risk for COVID-19.
- COVID-19 patients with SUDs are more likely to require hospitalization and to die from COVID-19 than those without SUD, with patients with OUD and African American patients at greatest risk.
One of the most common symptoms associated with coronavirus disease 2019 (COVID-19), which is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is impaired lung function. People with substance use disorders (SUDs) also frequently have diminished lung function or are at risk for respiratory depression from opioid use. Therefore, it had been hypothesized early in the COVID-19 pandemic that people with SUDs may be particularly vulnerable to COVID-19 and its most severe health outcomes. A recent analysis of health records confirms this assumption. “It is clear from our analysis that people with SUDs are indeed at higher risk of contracting and suffering worse consequences from COVID-19. This is especially true for African Americans,” says Dr. Nora D. Volkow, Director of NIDA and senior author of the study.
Electronic Health Records Show Increased COVID-19 Risk in People With SUDs
Dr. Volkow and her collaborators, Drs. Quan Qiu Wang and Rong Xu from Case Western Reserve University as well as Dr. David C. Kaelber from the MetroHealth System in Cleveland, Ohio, analyzed electronic health records of more than 73 million patients at 360 U.S. hospitals. About 10 percent of these patients (7.5 million) had been diagnosed with an SUD at some time in their lives, including alcohol use disorder, tobacco use disorder, cocaine use disorder, cannabis use disorder (CUD), or opioid use disorder (OUD).

Among all patients whose data were analyzed, 12,030 had been diagnosed with COVID-19. People who had ever had an SUD were significantly overrepresented in this group, making up about 16 percent of the COVID-19 patients compared with about 10 percent of the total sample. At the same time, people with a lifetime SUD diagnosis were 1.5 times more likely to develop COVID-19 than were people without SUD. COVID-19 risk also depended on the specific SUD diagnosis (see Figure 1). People with a lifetime diagnosis of OUD had the highest risk, and those with a lifetime diagnosis of CUD had the lowest risk, of COVID-19.
COVID-19 risk was particularly high among those with a recent SUD diagnosis (i.e., within the past year); their risk was more than 8 times higher than that of people without a recent SUD. Again, risk depended on the specific SUD. People with a recent OUD diagnosis were about 10 times more likely than people without recent SUDs to have COVID-19, whereas people with a recent CUD diagnosis were about 5 times more likely to have the disease.
The team also noted that African Americans with a recent SUD diagnosis were twice as likely to develop COVID-19 as were Caucasians. Risk was increased across all subtypes of SUD, with the largest effect seen among African Americans with a recent OUD diagnosis, who were 4 times more likely to have COVID-19 than Caucasians with a recent OUD diagnosis.
People With SUDs Had Worse Outcomes of COVID-19
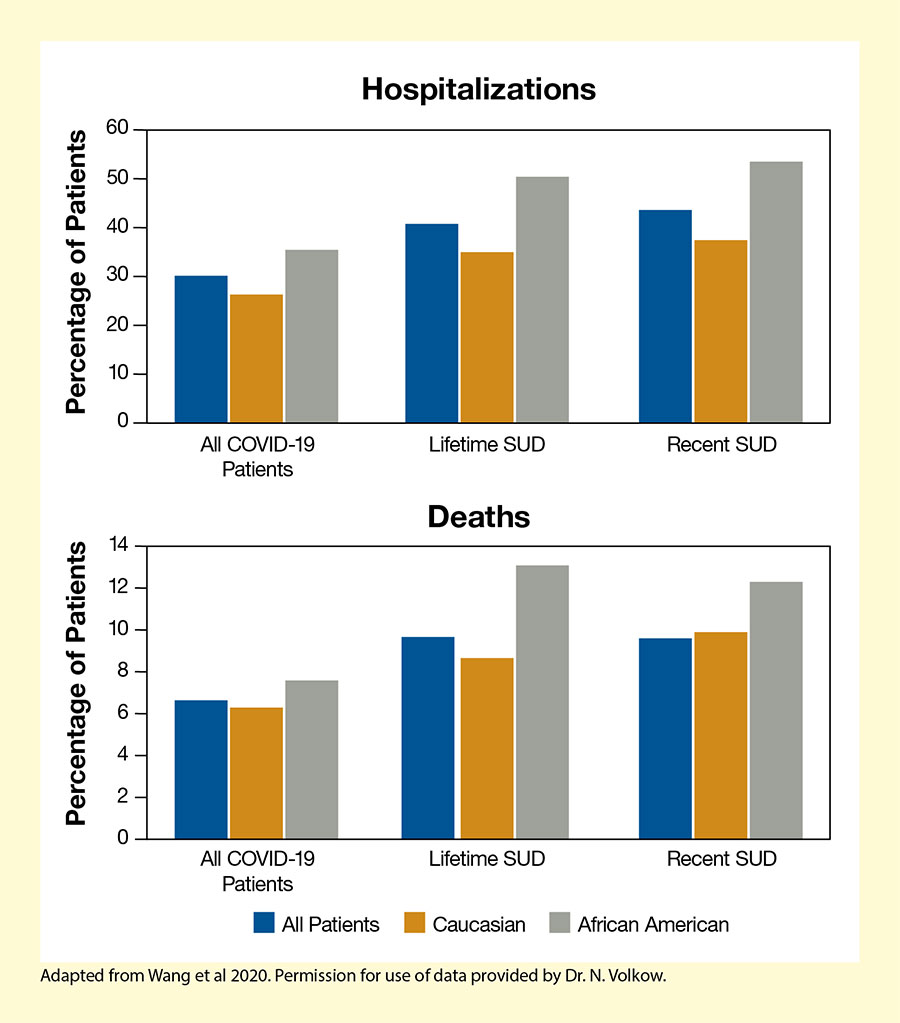
People with SUDs also had an increased risk of severe outcomes of COVID-19 (see Figure 2). More than 40 percent of COVID-19 patients with lifetime or recent SUD diagnoses required hospitalization, compared with 30 percent among all COVID-19 patients in the study. Similarly, a larger proportion of people with SUD diagnoses died from COVID-19 (about 10 percent) compared with all studied patients (about 7 percent). However, hospitalization and death risk did not differ between those with a recent SUD diagnosis and those with a lifetime diagnosis.
African Americans were disproportionately affected by COVID-19–related hospitalizations and deaths. Among African Americans with a lifetime SUD diagnosis, more than 50 percent required hospitalization and about 13 percent died, compared with about 35 percent and less than 9 percent, respectively, among their Caucasian counterparts.
Multiple Factors May Contribute to Increased Risk
Dr. Volkow and her colleagues speculate that multiple factors may increase risk for COVID-19 infection and adverse outcomes in people with SUDs. First, chronic substance use can harm or weaken the body by impairing heart and lung function or enhancing vulnerability to infection through other pathways. Chronic use of alcohol, tobacco, and other drugs also promotes development of conditions such as hypertension or diabetes that are associated with a more severe course of COVID-19.
Second, behaviors associated with use of opioids and other illicit drugs (e.g., interactions with people who use or deal drugs without regard to social distancing) may increase the risk of contracting infectious diseases, including COVID-19. Third, people with SUDs often experience barriers to health care access that put them at greater risk of adverse outcomes.
The impact of COVID-19 is particularly dramatic for African Americans with SUDs, who had a disproportionately high number of COVID-19 diagnoses as well as more severe outcomes. The researchers speculate that factors such as health care disparities, lower socioeconomic status, as well as higher rates of coexisting conditions that raise susceptibility to COVID-19 (e.g., hypertension, diabetes, cardiovascular diseases, and kidney diseases) may contribute to the increased vulnerability.
Dr. Volkow concludes, “Given what we now know about SUDs and COVID-19 susceptibility, it is crucial for providers to screen patients who have or are suspected of having COVID-19 for SUDs and smoking/vaping history. This is especially true for African Americans, for whom SUDs may confer special vulnerability for COVID-19 as a result of longstanding disparities in health and health care access.” She also notes that addressing SUDs should be part of any comprehensive public health approach to addressing COVID-19.
- Text Description of Figure 1
-
The bar chart illustrates the increased in risk of COVID-19 in people with lifetime and recent SUDs compared with people without SUDs. The left set of bars shows increased risk for people with an SUD at some time in their lives, while the right set of bars represents people with a recent SUD—that is, within the past year. Green bars represent people with any SUD, light blue represents people with opioid use disorder, orange represents people with tobacco use disorder, gray represents people with alcohol use disorder, purple represents people with cocaine use disorder, and dark blue represents people with cannabis use disorder. The vertical y-axis shows the increase in risk compared with people without an SUD on a scale from 0 to 12.
Among those with a lifetime diagnosis of an SUD, risk was increased about 1.5 times among those with any SUD, about 2.4 times among those with opioid use disorder, about 1.3 times among those with tobacco use disorder, about 1.4 times among those with alcohol use disorder, about 1.6 times among those with cocaine use disorder, and about 0.9 times among those with cannabis use disorder. Among those with a recent SUD diagnosis, risk was increased about 8.7 times among those with any SUD, about 10.2 times among those with opioid use disorder, about 8.2 times among those with tobacco use disorder, about 7.6 times among those with alcohol use disorder, about 6.5 times among those with cocaine use disorder, and about 5.3 times among those with cannabis use disorder.
- Text Description of Figure 2
-
The bar charts show the percentage of patients who required hospitalization or died among all COVID-19 patients (left set of bars), COVID-19 patients with a lifetime SUD (middle set of bars), and COVID-19 patients with a recent SUD (right set of bars). Blue bars represent all patients, orange bars represent Caucasian patients, and gray bars represent African American patients in each group.
The upper panel shows hospitalizations among COVID-19 patients. The vertical y-axis shows the percentage of patients requiring hospitalization on a scale from 0 to 60. Among all COVID-19 patients, the rate of hospitalization was 30 percent for the entire sample, about 26 percent for Caucasians, and about 36 percent for African Americans. Among COVID-19 patients with a lifetime SUD, the rate of hospitalization was about 40 percent for the entire sample, about 35.2 percent for Caucasians, and about 50 percent for African Americans. Among COVID-19 patients with a recent SUD, the rate of hospitalization was about 44 percent for the entire sample, about 38 percent for Caucasians, and about 55 percent for African Americans.
The lower panel shows death rates among COVID-19 patients. The vertical y-axis shows the percentage of patients who died on a scale from 0 to 12. Among all COVID-19 patients, the death rate was 6.6 percent for the entire sample, about 6.2 percent for Caucasians, and about 7.5 percent for African Americans. Among COVID-19 patients with a lifetime SUD, the death rate was about 9.6 percent for the entire sample, about 8.6 percent for Caucasians, and about 13.0 percent for African Americans. Among COVID-19 patients with a recent SUD, the death rate was about 9.5 percent for the entire sample, about 9.8 percent for Caucasians, and about 12.2 percent for African Americans.
Source:
- Wang, Q.Q., Kaelber, D.C., Xu, R., and Volkow, N.D. COVID-19 Risk and Outcomes in Patients With Substance Use Disorders: Analyses From Electronic Health Records in the United States. Molecular Psychology 2020. DOI: 10.1038/s41380-020-00880.