
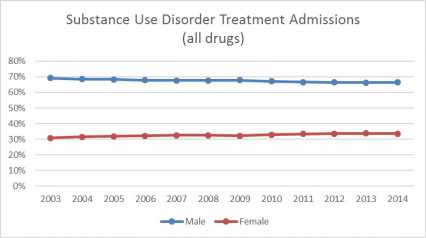
There are more men than women in treatment for substance use disorders. However, women are more likely to seek treatment for dependence on sedatives such as anti-anxiety and sleep medications.14 In addition, although men have historically been more likely to seek treatment for heroin use, the rate of women seeking treatment has increased in recent decades.154
Substance use disorders may progress differently for women than for men. Women often have a shorter history of using certain substances such as cocaine,155 opioids,42 marijuana,42,43,156 or alcohol.42,157,158 However, they typically enter substance use disorder treatment with more severe medical, behavioral, psychological, and social problems. This is because women show a quicker progression from first using the substance to developing dependence.159
Substance Use Disorder Treatment Admissions (all drugs)
Many women who are pregnant or have young children do not seek treatment or drop out of treatment early because they are unable to take care of their children; they may also fear that authorities will remove their children from their care. The combined burdens of work, home care, child care, and other family responsibilities, plus attending treatment frequently, can be overwhelming for many women. Successful treatment may need to provide an increased level of support to address these needs.7
Women and Smoking Cessation Treatment

Research shows that women are less likely to try to quit smoking and more likely to relapse if they do quit.90 Nicotine-replacement options, such as the patch or gum, are not as effective for women as for men, and nicotine withdrawal may be more intense for women.160,161 Nicotine craving162 and withdrawal163 vary across the menstrual cycle, which may further complicate a woman's attempts to quit.
Some women continue to smoke because they are afraid they will gain weight. However, research shows only a modest weight gain after quitting. The average smoker gains 6 to 10 pounds after quitting smoking, but certain diet and lifestyle changes can reduce the risk of weight gain. If a person does gain weight, the average person loses much of the extra weight within 6 months.164 In fact, long-term quitters gain, on average, only 2 pounds.165 Most importantly, the health benefits of quitting smoking far exceed the risks of gaining a few pounds. Quitting also decreases risks for various types of cancers, heart attack, and lung disease.164
Substance Use Disorder Treatment for Mothers and Their Babies While Pregnant or Breastfeeding
A pregnant woman should ask for medical help to stop her drug use. If she attempts to suddenly withdraw from addictive drugs and alcohol without medical assistance, she could be putting her fetus at risk.166
Intensive outpatient treatment, which provides a higher treatment level than traditional outpatient programs but does not require structured residential living, has produced positive results for pregnant women. Pregnant women are more likely to stay in these treatment programs if they provide services such as child care,168 parenting classes, and vocational training.169,170
In addition, it is important to monitor newborns of substance-using mothers for symptoms of withdrawal and provide proper treatment if necessary. Treatment of drug dependency in newborns depends on the severity of symptoms and, while nonpharmacological treatments are preferred, it sometimes may include hospitalization in order to receive intravenous fluids and medications. These medications are gradually tapered off until the infant adapts to being drug-free.
Treating Opioid Use Disorders in Pregnant Women
Pregnant women who are addicted to opioid pain relievers or heroin face special problems because the baby can be born dependent. Currently, the U.S. Food and Drug Administration has not approved medications to treat opioid-dependent pregnant women, but methadone or buprenorphine maintenance combined with prenatal care and a comprehensive drug treatment program can improve many of the adverse outcomes associated with untreated opioid use disorder.166,171 In general, it is neither recommended nor necessary for pregnant women to cease methadone or buprenorphine treatment.167,171 However, newborns exposed to methadone during pregnancy can require treatment for withdrawal symptoms.
Some studies suggest that buprenorphine (Suboxone®, Subutex®) has some advantages over single-dose methadone as a treatment for opioid use disorder in pregnant women. Infants born to mothers treated with buprenorphine had fewer symptoms of dependence and reduced length of hospital stay compared to those treated with methadone.172
Pregnant women who take buprenorphine for opioid use disorder during pregnancy should be aware that the amount of buprenorphine passed through breast milk may be inadequate to prevent opioid withdrawal in their infant. In some cases, treatment of the infant may be required.173
Pregnant women who are addicted to opioids, even if they are in treatment, should monitor their babies for drowsiness, inadequate weight gain, and failure to meet developmental milestones—especially in younger, exclusively breastfed infants. Although unlikely, if a breastfed baby of a woman on buprenorphine therapy shows signs of increased sleepiness, difficulty feeding or breathing, or limpness, a health care provider should be contacted immediately. Infants should be observed for withdrawal signs if breastfeeding is abruptly stopped.173
As for infants born with NAS due to opioids, recovery can require hospitalization and possibly treatment with morphine or methadone to relieve symptoms;94 researchers have also studied buprenorphine for this purpose.174 There is some evidence that buprenorphine is superior to morphine in treating infants with opioid-related NAS. A NIDA-funded study published found that treating NAS babies with sublingual buprenorphine resulted in a shorter duration of treatment than oral morphine. It also resulted in a shorter length of hospital stay, with similar rates of adverse events.175